Fibrates
Examples
- Bezafibrate
- Fenofibrate
Indications
- Second line treatment for primary and secondary prevention of cardiovascular disease where a statin is not tolerated
Contraindications
Contraindications:
- Pregnancy and breast feeding
- Patients with severe hepatic insufficiency
- Primary biliary cirrhosis or gall bladder disease
- Nephrotic Syndrome
- Patients with Hypothyroidism require active management before starting therapy with a fibrate
- Use with caution in renal impairment
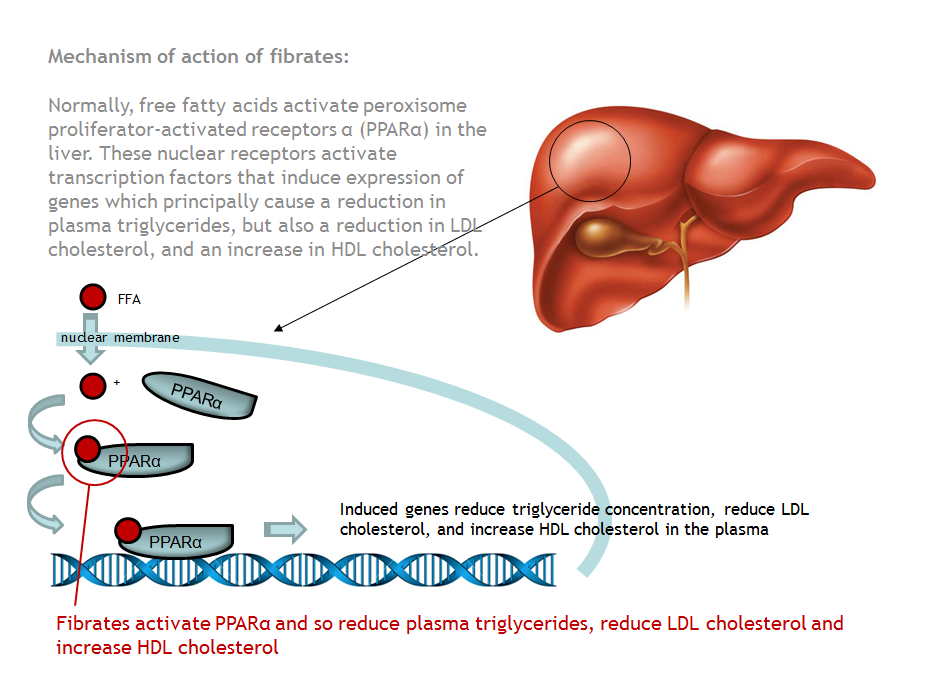
Mechanism
Fibrates work by stimulating PPARα (peroxisome proliferator-activated receptor alpha), which produces a range of effects on lipid metabolism. Most importantly, fibrates cause a significant fall in the concentration of plasma triglycerides (can achieve a 30% reduction). In addition, they cause a decrease in LDL cholesterol (approximately 10%) and a rise in HDL (approximately 10%).
Administration
Oral.
Adverse Reactions
Myositis, this is uncommon but can be fatal. Patients will develop symptoms of muscle pain and stiffness and can progress to rhabdomyolitis. If patients develop muscle pains measure creatine kinase urgently and stop treatment. This is more likely in patients with impaired renal function and those who are given concurrent Statins.
Gastrointestinal disturbance: nausea and vomiting are common.
Gastrointestinal disturbance: nausea and vomiting are common.
Interactions
Concomitant treatment with Statins and Ciclosporin increase the risk of developing myositis.
Fibrates enhance the anticoagulant effect of warfarin.
There is an increased risk of hypoglycaemia when insulin or sulfonylureas are given with fibrates.
Fibrates enhance the anticoagulant effect of warfarin.
There is an increased risk of hypoglycaemia when insulin or sulfonylureas are given with fibrates.
Education
Advise the patent to report any signs of myopathy / myositis immediately. These include generalised muscle weakness, pains or tenderness.
Patients concurrently on warfarin need to ensure they attend for regular INR monitoring.
Patients concurrently on warfarin need to ensure they attend for regular INR monitoring.
Pharmacokinetics
No specific issues
