Statins
Examples
- Simvastatin
- Atorvastatin
- Rosuvastatin
- Pravastatin
Indications
- Patients with hyperlipoproteinaemia (i.e. a total serum cholesterol concentration to HDL cholesterol ratio > 6 mmol/L) eg those with Familial hypercholesterolaemia.
- Primary prevention of coronary events in patients at increases risk of coronary heart disease
- Secondary prevention of cardiovascular events
Contraindications
Contraindications:
- Acute liver disease / persistently abnormal liver function tests
- Pregnancy and breast feeding - statins are teratogenic. Women should avoid becoming pregnant whilst taking statins and for 1 month after stopping treatment
- Porphyria
- Patients with renal insufficiency
- Patients with high alcohol intake
- Patients with risk factors for myositis / rhabdomyolysis
- Patients with hypothyroidism require active management before starting therapy with a statin (hypothyroidism may increase the risk of myositis)
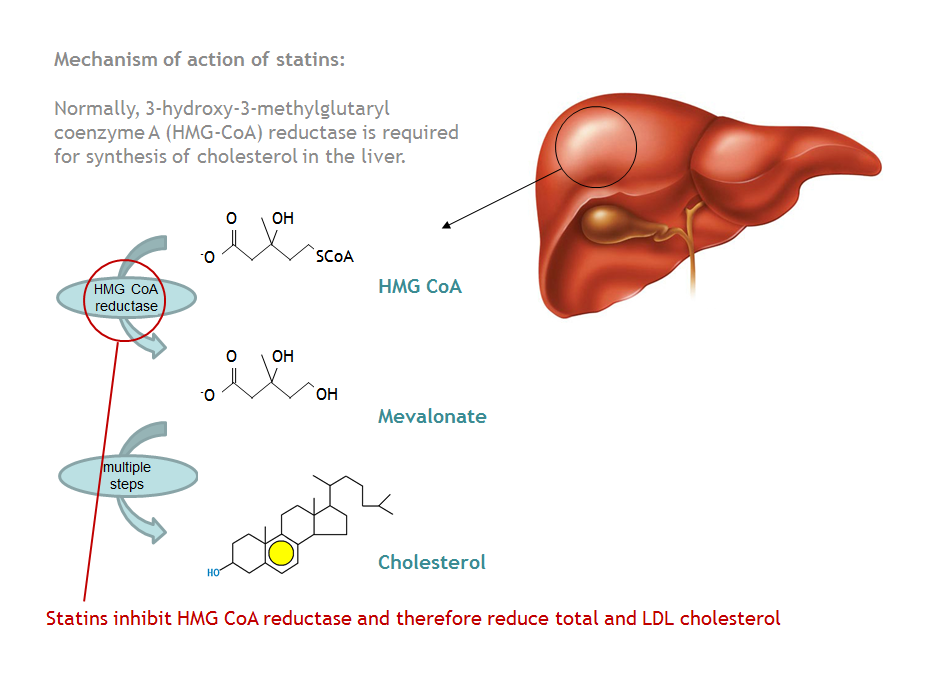
Mechanism
Statins competitively inhibit 3-hydroxy-3-methyglutaryl co-enzyme A (HMG-CoA) reductase. This enzyme is required for cholesterol synthesis in the liver. A fall in hepatocyte cholesterol synthesis causes an increase in hepatic LDL receptors, causing an increase in cholesterol clearance and therefore a fall in total and LDL plasma cholesterol. Statins are more effective at lowering LDL- cholesterol concentration than other lipid lowering agents e.g. fibrates, however they are less effective at reducing triglyceride concentration.
Administration
Oral, daily dose to be taken at night (simvastatin and pravastatin only. Statins with longer half-lives can be taken at any point during the day e.g. atorvastatin and rosuvastatin). Before starting treatment measure the cholesterol level, measure again after several months and adjust the dose based on current cholesterol targets.
Adverse Reactions
- Myositis / Myopathy - patients will develop muscle pain, tenderness and stiffness. The condition is reversible if the statin therapy is withdrawn. This condition is rare but can be fatal
- A transient rise in creatinine kinase is often seen (usually occurs in the first 3 months). Statin therapy must be stopped if the rise is > 3x normal or baseline CK
- Gastrointestinal disturbance; abdominal pain, diarrhoea, flatulence and vomiting
- Hepatitis, rare but important
- Measure liver function tests before stating treatment, after 1-3 months and at 6-12 months
Interactions
Increased risk of myositis and rhabdomyolysis if statins are prescribed with:
Grapefruit can also increase patient exposure to atorvastatin or simvastatin
- Fibrates
- Ciclosporin
- Macrolides
- Azole anti-fungals
- Calcium channel blockers
Grapefruit can also increase patient exposure to atorvastatin or simvastatin
Education
Advise the patient to report any signs of myopathy / myositis immediately. These include generalised muscle weakness, pains or tenderness.
All patients should also be on a diet and exercise regime. Efforts should be made to modify other cardiovascular risk factors.
Patients concurrently on warfarin need to ensure they attend for regular INR monitoring.
All patients should also be on a diet and exercise regime. Efforts should be made to modify other cardiovascular risk factors.
Patients concurrently on warfarin need to ensure they attend for regular INR monitoring.
Pharmacokinetics
No specific issues
