Angiotensin II Receptor Blockers (ARB's)
Examples
- Losartan
- Irbesartan
Indications
- Hypertension
- Post MI, secondary prevention
- Heart failure
- Diabetic nephropathy
Contraindications
Contraindications:
- Pregnancy - ACE-i have a teratogenic effect
- Bilateral renovascular disease - ACE-i can cause severe renal impairment
- Severe renal failure
- Hepatic insufficiency
- Patients with a fixed cardiac output (e.g. aortic stenosis, mitral stenosis and hypertrophic cardiomyopathy) - ACE-i cause vasodilatation and in these patients a significant fall in blood pressure can occur
- Breast feeding
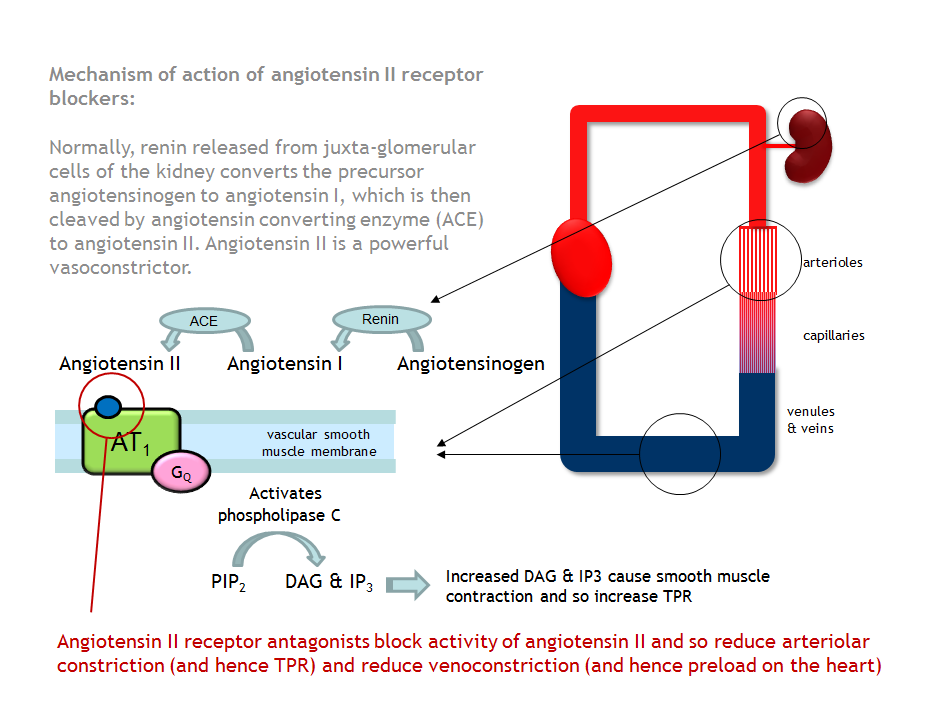
Mechanism
Angiotensin II Receptor Antagonists block Angiotensin II at the type 1 subtype of the Angiotensin II (AT1) receptor. The vasoconstricting properties of Angiotensin II are therefore blocked causing relative systemic vasodilatation.
The effects of Angiotensin II receptor blockers are similar to those of ACE-i. The advantage of ARB's is unlike ACE-i they do not interfere with the breakdown of bradykinin and therefore do not cause a cough. This makes them a useful alternative treatment in some patients.
Administration
Oral
Check patient's urea and electrolytes before and 1-2 weeks after starting treatment. This should identify whether the patient's renal function has been impaired and would lead to discontinuation of the drug and further investigation of the kidneys.
Check patient's urea and electrolytes before and 1-2 weeks after starting treatment. This should identify whether the patient's renal function has been impaired and would lead to discontinuation of the drug and further investigation of the kidneys.
Adverse Reactions
- Renal impairment
- As with ACE-i, symptomatic hypotension can occur
- Hyperkalemia (rare if used as a single therapy). A reduction in Angiotensin II causes a fall in Aldosterone secretion (Aldosterone increases Na+ reabsorption and K+ excretion) leading to a rise in K+
- Although angioedema is thought to be due to ACE-i effect on bradykinin, there have been case reports of angioedema also occurring in patients on ARBs (normally following this side effect with an ACE-i)
Interactions
A pharmacodynamic interaction can be seen between ARBs and any medication which can also reduce GFR (commonly NSAIDs or diuretics).
Loop diuretics and ARBs can cause hypotension as diuretic therapy will deplete the intravascular volume. In some patients it may be desirable to temporarily stop treatment with diuretics before starting an ARB. In other patients, the synergistic effect on blood pressure may be desirable.
Loop diuretics and ARBs can cause hypotension as diuretic therapy will deplete the intravascular volume. In some patients it may be desirable to temporarily stop treatment with diuretics before starting an ARB. In other patients, the synergistic effect on blood pressure may be desirable.
Education
Warn patients about the adverse reactions, in particular first dose hypotension.
If the indication for use is hypertension, inform the patient about the importance of having their blood pressure checked regularly.
If indicated inform the patient about the importance of having their blood tested to assess their renal function and electrolyte status.
If the indication for use is hypertension, inform the patient about the importance of having their blood pressure checked regularly.
If indicated inform the patient about the importance of having their blood tested to assess their renal function and electrolyte status.
Pharmacokinetics
No specific issues
