STEMI and NSTEMI
ST Elevated Myocardial Infarction and Non-ST Elevated Myocardial Infarction
Learn about the cardinal features of these two types of myocardial infarction and also the appearance of asystole
Normal Rhythm:
where the SA node depolarises first which then conducts to the AV node, down the Bundle of His and through the left and right bundle branches to the purkinje fibres.
Compare the other ECG tracings to this normal one.
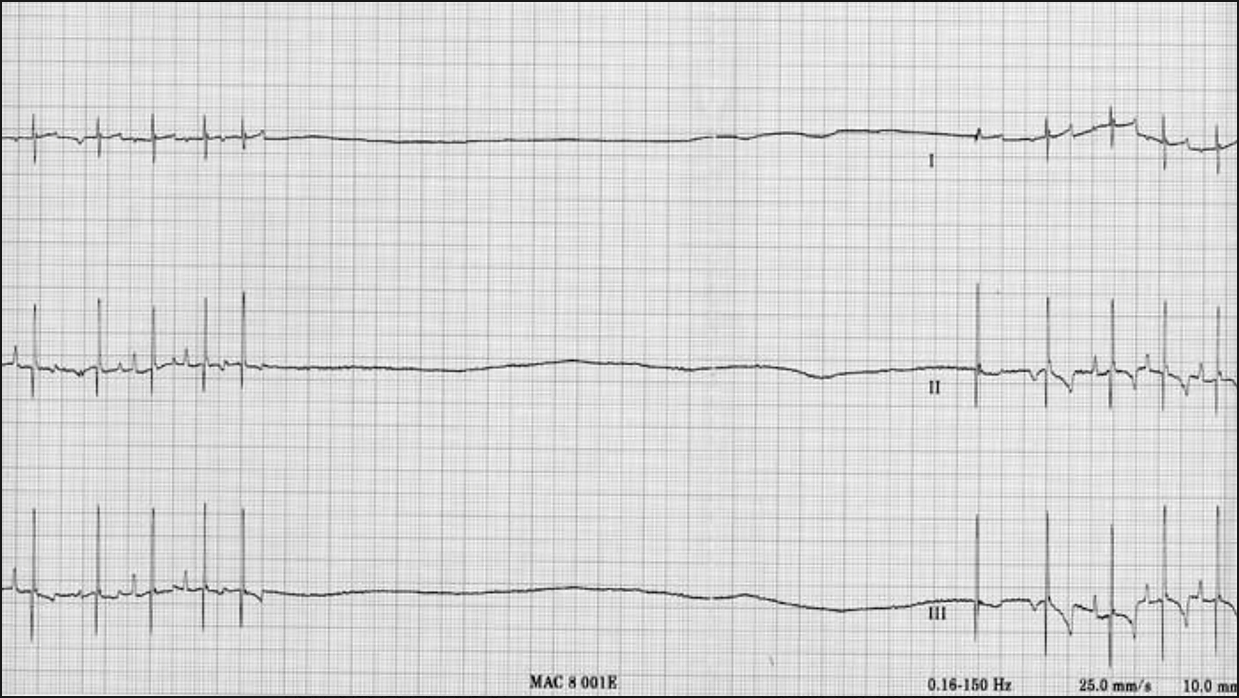
Asystole:
This is where there is a lack of any contraction in the ventricles and subsequently there is a period of no electrical activity (flat line) on the ECG.
It normally occurs from degeneration from ventricular fibrillation when the myocardium eventually runs out of energy and stops fibrillating altogether. However this is not the case in this ECG.
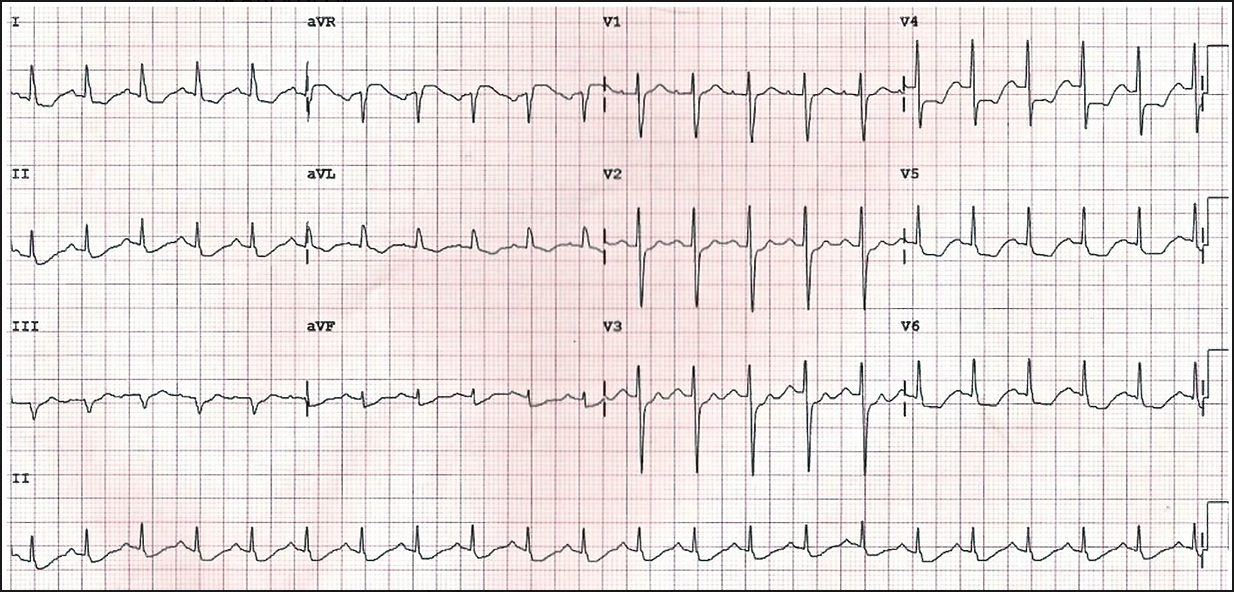
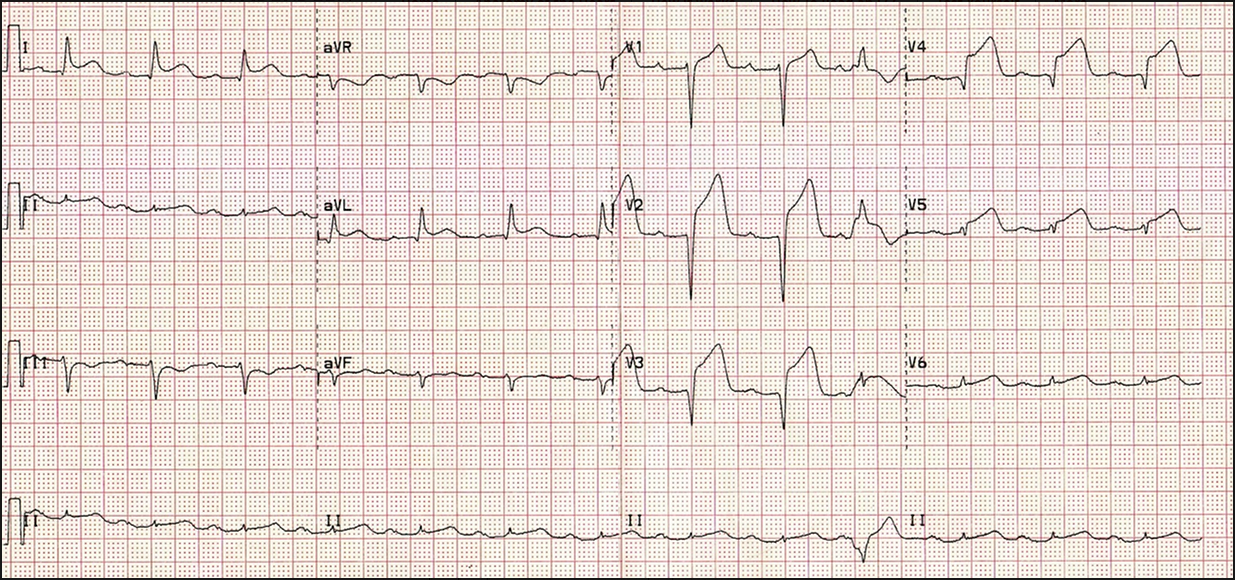
Anterior MI:
This happens due to occlusion of the left anterior descending coronary artery
Look at the chest leads V1-6. There is elevation in the ST segment for each of these.
This suggests that the MI has occurred in the anterolateral segment of the heart since the anterior leads V3 and 4 as well as the lateral leads V5 and 6 have the most marked elevation.
NOTE: there is also reciprocal ST depression in the inferior leads, mainly III and aVF

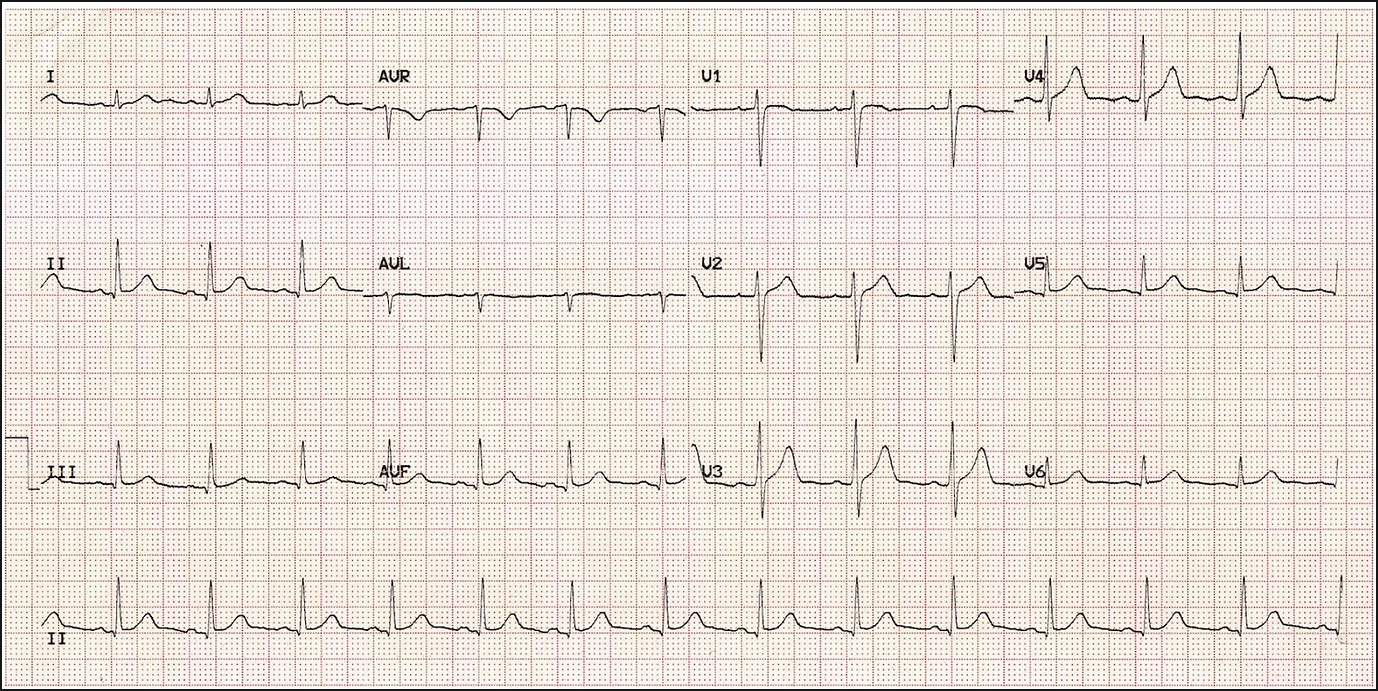
Lateral MI:
Here branches of the left anterior descending and left circumflex arteries have been affected.
There is ST elevation in the lateral leads (I, aVR V5 and V6).
There is reciprocal ST depression in the inferior leads III and aVF
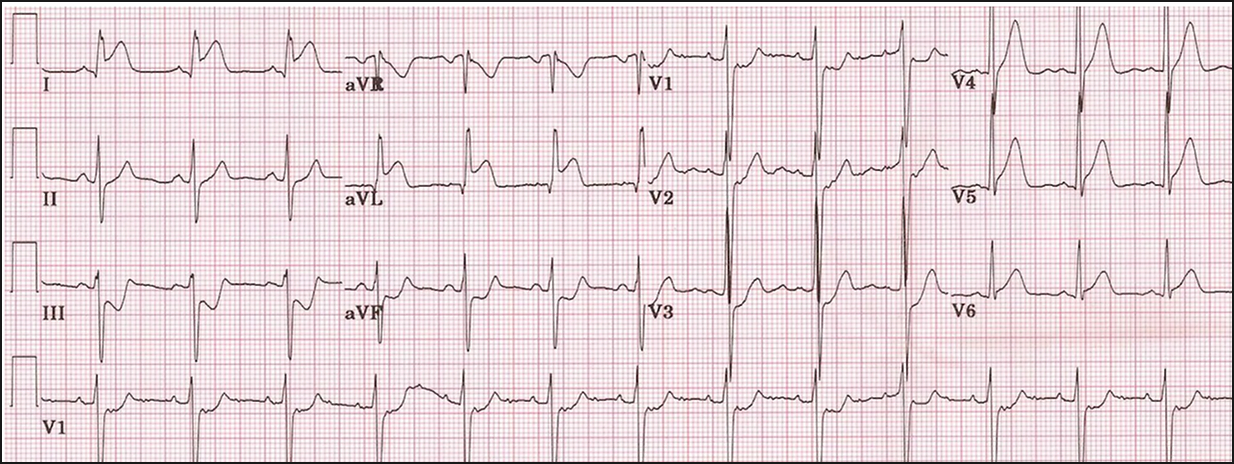
Septal MI:
ST elevation in leads V1 and 2 suggesting a septal MI.
However there is also ST elevation in V3-6 and so other areas of the heart are involved as well
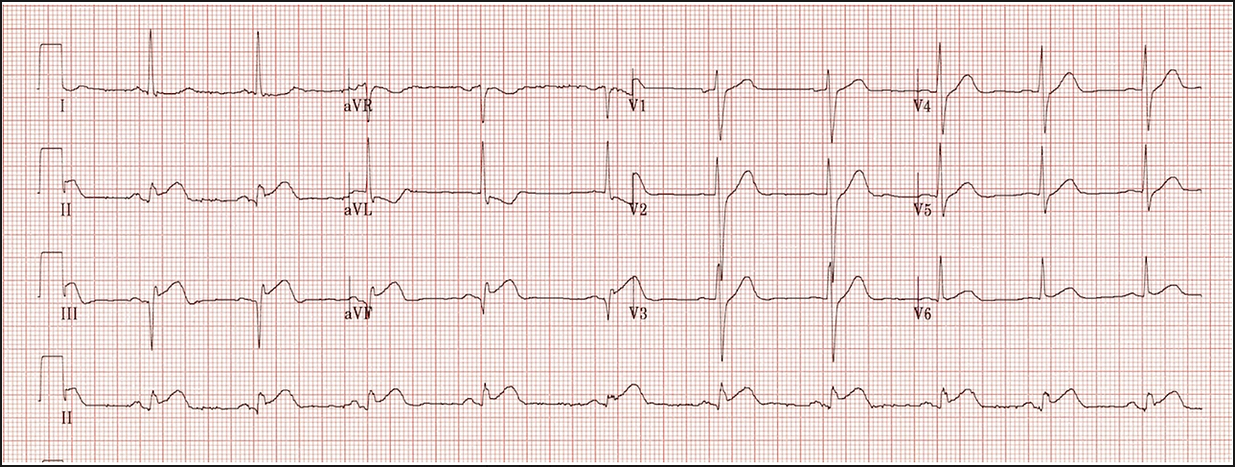
Inferior MI:
This can result from blockage of the right coronary artery. Less commonly it is due to blockage of the left circumflex artery.Because the SAN and AV nodes are supplied by the RCA heart blocks are more common in inferior MIs
There is ST elevation in the inferior leads (II, III, aVF) and there is reciprocal ST depression in lead I and aVL
NSTEMI and Ischaemia:
This is an ECG of an NSTEMI or unstable angina. In lots of the leads ST segment depression can be seen which suggests ischaemia.
This can progress to a STEMI where ST elevation can be seen as well as other features like T-wave inversion