What is Clearance? - Renal Clearance
Some drugs are totally excreted unchanged in the urine, while others are extensively metabolised, usually within the liver, before being excreted. It is important to know which route of elimination predominates for an individual drug because this allows prescribers to anticipate its susceptibility to drug interactions involving drug metabolism and any dose adjustment that may be necessary when eliminating organ function is impaired.
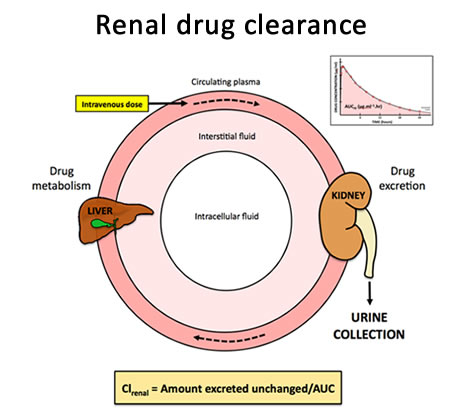
Like hepatic clearance, renal clearance (Clrenal) relates plasma concentration to the rate of excretion:
In practice, renal drug clearance is difficult to estimate from urine and plasma concentration data (as for creatinine clearance) because plasma concentration is falling exponentially throughout the period of excretion. It can be estimated by relating the total amount of drug excreted unchanged and the total area under the plasma concentration-time curve (AUC) (Fig 8), as follows:
However, this method is practical only for drugs with relatively short half-lives where the collection period is not prolonged over several days. Alternatively, if the fraction of the total dose that is collected unchanged in the urine after an intravenous dose (fe) and total clearance (Cltotal) are known then renal clearance can be calculated:
